Dr. Andrew's Corner
Get the Latest Education
Dr. Andrew's Corner

The History of VacuMetrics, Inc.
(Including VacuMed, a division of Vacumetrics Inc.)
Vacumetrics Inc., was founded in 1968 by John Hoppe in Waltham, Massachusetts. The company's goal was to develop a mass spectrometer for pulmonary gas analysis and mass spectrometer accessories in general.
The company introduced its first commercial mass spectrometer in 1970. In 1972, Statham Instruments of Oxnard, California acquired Vacumetrics and moved the company and its key employees to Oxnard. Two years later, Gould Inc., in turn, acquired Statham Instruments and sold the mass spectrometer product line.
In 1974, John Hoppe started a new company in Ventura, California called, again, Vacumetrics Inc. VacuMed is a division of Vacumetrics, Inc., specializing in medical instrumentation and supplies.
The company manufacturers approximately 50% of the products it sells and acts as a distributor for the balance. VacuMed distributes products worldwide. You may order direct from VacuMed or from one or our distributors located worldwide.
Metabolic Simulation & Testing Systems
Helpful Hints for Setting up an
Exercise Stress Testing Laboratory
(C) Copyright VacuMed 1998 - 2006
When most lay people hear the word STRESS TEST, they visualize a person running on a treadmill or pedaling on a stationary bicycle while all kinds of wires are attached.
What they think of is the Cardiac Stress Test.
It is not immediately obvious to everyone, that a deficiency in the performance of the heart may be caused by an insufficiency of the lung. So we now know that a Stress Test may mean either, or both, a Cardiac and/or Pulmonary evaluation.
Cardiac Stress testing in a clinical setting is fairly well understood and the equipment required is well known. This is not necessarily so for Pulmonary Stress Testing.
Simple, computerized equipment for pulmonary stress testing (gas exchange analysis) has only become available since the introduction of the Personal Computer (PC). Prior to that, it was a cumbersome procedure requiring the collection of exhaled gases in Douglas bags or large Tissot spirometers and then determining the gas concentrations by various gas analysis instruments.
Pulmonary stress test systems go by a number of names: VO2 Measurement System, Metabolic Cart, CPX System, or Ergospirometry System as they are called in Europe.
To keep it short, we will use CPX hereafter.
Now, a number of companies offer automatic and computerized data acquisition and analysis.
While a cardiac stress test is almost exclusively conducted for the purpose of evaluating a problem or suspected problem with the heart, there are several reasons for measuring oxygen consumption:
- To test a patient with a suspected illness or deficiency
- To measure the progress of "Rehab"
- To measure the progress of a weight loss program
- Fitness Evaluation: Physical performance of athletes
- Nutritional assessment
Perhaps the most important differences we find between labs testing "patients" vs. labs testing so-called "normal" subjects is the use of the 12-lead ECG and the availability of resuscitation equipment and personnel trained in it's use.
2. Equipment for the Cardiac Stress Test
The equipment required is usually obvious and well understood, but you should be aware that there is a big price differential between Resting ECG and Stress Testing ECG. In evaluating competing systems, be sure you understand software options, such as "Full Disclosure", "Automatic Arrhythmia Detection", "ST Segment Analysis" and others, which may affect the cost of the system.Minimum requirements are a 12-lead system with STRESS TEST software.
See ECG Menu
Other equipment required:
Exercise Devices: Treadmills or ergometer , more details in chapter 5.
Blood pressure sphygmomanometer (e.g. Baumanometer) or
Electronic non-invasive blood pressure meter, see VacuMed number "Tango"
Emergency Resuscitation Equipment
Defibrillator
Crash cart, Ambu bags, 100% oxygen with face mask,
Resuscitation mask, e.g. CPR Micro Shield
3. Equipment for the Pulmonary Stress Test Lab
The instrumentation here can vary greatly depending on the type of testing to be performed, the reason for the test, the mission of the laboratory and the desired accuracy. For example, a college teaching laboratory might be more interested in a basic low cost system, while a lab planning to publish their findings would be more interested in accuracy. Listed in approximate order of importance- Oxygen Consumption (VO2, VCO2) Measurement System (or CPX)
- Calibration Gases & Pressure Regulators Should include a true "Zero" gas, usually 100% N2 and a "Span" gas, such as 16% O2 and 4%CO2.
- Calibration Syringe , usually a 3-liter volume syringe
- Exercise Device: Treadmills , Ergometers , rowing machine, etc.,
more details in chapter 5. - Patient Interface:
a. Mouthpiece , 2-way valve and nose clip
b. Stress Test Face Mask with headgear
Consider the V-Mask or Air Cushion Masks ("KM-Mask") - Heart Rate Measurements or EKG system One channel (3-lead) minimum
- Barometer
- Hygrometer and Thermometer to measure relative humidity
- Metabolic Calibrator / Simulator
- Spirometer
- Lactate Analyzer
- Weight Scale and Height Measure
- Valve Balancer, hangs breathing valve from overhead support
- Body fat Measurement Method:
The Gold Standard: Underwater Weighing System
Electronic Systems: Impedance measurements
Body fat Calipers - Metronome: For use when the exercising subject needs to maintain a steady cadence (Such as when using non-isopower ergometer).
4. The VO2 System: What to look for
All CPX's (VO2 Measurement Systems) contain the same basic building blocks:Oxygen and CO2 analyzers, a ventilation measurement device, interfacing electronics, gas sampling system, data acquisition system and some kind of computer and software.
Most CPX manufacturers do not make their own gas analyzers, instead they buy them from companies that specialize in making nothing but gas analysis equipment. This is actually good news, because better quality can often be achieved by specialization.
The other major component is the ventilation measurement device or flow sensor. The chart below may help you select a desirable flow sensor.
Almost all companies use a PC now, so very little differentiation can be expected there.
The final and perhaps most important component is the software. It is the software that ultimately determines the accuracy of the VO2 measurement. You may have the world's best gas analyzers, but if the software does not correctly align gas data with flow data, or if the compensation for barometric pressure, temperature and humidity is not handled correctly, then the system cannot report accurate VO2's.
To our knowledge only a Metabolic Simulator(1,2) can accurately verify if the system operates correctly.
Here are some other questions you may want to ask before you buy:
- Can you look at a demo disk of the software before you buy?
- Can the system be interfaced to a notebook computer in case you need a portable system?
- If you need options such as EtCO2 or SAO2, are they available, can they be added later?
- Is software available for test interpretation, data base analysis or exercise prescription?
5. Exercise Devices
There are a lot of exercise devices on the market and this listing is not intended to be complete.Treadmills
In our opinion, for testing you should not consider a treadmill costing less than $4000. The desirable, higher priced machines should include motorized elevation, built-in and programmable exercise protocols and/or the ability to be remotely programmed by your stress test software.VacuMed's models 13610 and 13620 meet this description and also include a "Kill Switch" that automatically shuts of the treadmill if the runner gets too far away from the control console. Model 13610 is a heavy duty research type treadmill. Most manufacturers of exercise stress testing devices offer treadmills with their own name on them but manufactured by other companies specializing in treadmill manufacturing.
Ergometers
Ergometers, in principle, are more desireable for exercise stress testing because they allow the direct determination of braking power in watts, while treadmills only allow an indirect approximation. However, if you are testing runners, then a treadmill will be the preferred device.In our opinion, for CPX testing you should not consider an ergometer costing less than $2000. Ergometers are stationary bicycles that have some kind of braking mechanism that can be calibrated in Watts, Joules or KPM. Braking mechanisms using belts, brake pads tend to be less accurate. Modern braking mechanisms use electro-magnetic brakes (eddy current). For more advise on selecting ergometers, go back to Dr Andrew's Corner.
Rowing Machines and Stairclimber are sports-specific and are almost never used in a clinical setting.
6. Accessories & Supplies
Typical cardiac supplies:- ECG chart paper
- Electrodes
- Electrode Gel
- Skin Prep
- Stress Test Shirt
Keeps electrodes and electrode cables in place to minimizes movement artifacts. Bandages and tape to keep electrodes in place. Wipes to remove electrode gel after test.Basic emergency response supplies:
- Resuscitation mask, e.g. CPR Micro Shield
Typical pulmonary test supplies:
- Mouthpieces and Noseclips Note # 109NT mouthpiece works well with subjects wearing dental braces
- Nose clips , disposable Nose clip, permanent
- Breathing Tubes , to connect the exhalation valve to the mixing chamber. (In mixing chamber systems)
- Sample Tubing , to connect the gas sample port to the gas analyzer input 1/8" ID and 1/16" ID respectively (In breath-by-breath systems)
- Sterilizing/Disinfecting Solution to clean mouthpieces and breathing valves
- Silicone Grease to lubricate valve threads and tubing joints
- Pulmonary Function Test Filters
- Towels
- Drink: Access to drinking water or juice
- Capsaisin (available in the US as "Zostrix") promotes blood flow to the earlobe in case of problems with SAO2 or heart rate sensors.
(Read CAUTION label!)
7. Laboratory Setup
Make sure large equipment, such as treadmills and underwater weighing tanks will fit through doors, hallways or windows.
The layout should consider the number of people likely to be present during testing. In a teaching environment you may want a large number of students to witness the test. This may require secondary monitors to be placed in visible locations.
Do you want the test subject to see the computer screen during test?
Provide for adequate ventilation, install a fan in front of the test subject to cool him during exercise.
The laboratory should have a sink to wash hands, clean mouthpieces, masks, etc.
We have seen labs placing a mattress behind a treadmill to minimize injuries in case of a fall. A treadmill with a "Kill Switch" is a useful safety feature.
If you are using an ergometer, make sure the seat is adjusted high enough so the knee of the test subject is fully extended on the down stroke.
Place a RPE (Rate of Perceived Exertion) chart (if desired) within convenient reach of the test subject.
Prominently post instructions for emergency procedures, phone numbers for emergency assistance. Spell out instructions to emergency personnel how to find you.
Decide where your data files will be stored; institute computer backup procedures.
Verify the accuracy of your barometer by calling the local weather bureau or the nearest airport control tower, they have accurate instruments.
8. Test Precautions
Consult the publications listed on the next page.
Know the symptoms that require test termination.
Read the instruction manual that comes with your instruments.
Some additional comments:
Develop a questionnaire even for "normal" subjects to determine risk factors.
Conduct a simple spirometer test to detect respiratory impairment.
Tell your test subject to wear comfortable clothing, such as shorts and T-shirt, as well as walking or running shoes.
If you are using a treadmill, demonstrate how to get on and off the running treadmill.
Make sure tubing connections and electrode cables are secure to avoid having to repeat the test.
If you are using a face mask block off the exhalation port and ask the subject to pressurize the mask (exhale) to check for leaks.
Some people produce insufficient signals with earlobe SAO2 or heart rate sensors.
Keep some capsaicin (Zostix) on hand to apply to earlobe, but wash hands immediately to prevent getting it into eyes or other sensitive body areas.
9. What are the reasons for Exercise (CPX) Stress Testing
and what can you teach with a CPX System?
9.1 Exercise Physiology
Exercise requires the integration of physiological mechanisms to enable both, the respiratory and cardiovascular systems to support the increased metabolic demands.During exercise, both ventilatory and cardiovascular systems are under stress. The ability to respond adequately to this stress is a measure of physiological health and fitness.
Exercise testing evaluates the respiratory and cardiovascular responses to increased gradual workloads in order to define the level of physical work capacity, and to determine the limiting factors to the increased metabolic demands of exercise.
Serial exercise studies help define the effects of treatment or fitness programs on the physiological response to physical work.
Here are some examples of exercise related study subjects:
- Metabolism, Physiologic Responses to Various Stimuli: Exercise, diet or food groups.
- Respiratory Gas Exchange (VO2, VCO2), Oxygen debt, effect of CO2 retention (hypoventilation) on the regulation of CO2 stores in the body.
- Assessment of Physical Fitness: VO2max, Anaerobic (lactic) Threshold (AT or LT) as a percentage of VO2max. VO2 dynamics, t* (tau)
- Assessment of a Training or Weight Loss Program. Lowering of VCO2 and HR at a given exercise level as a result of training. Reduction of t for VO2 and VO2 drift for constant load heavy exercise.
- Progress of Post-Injury Rehabilitation. Improvement in VO2max, AT and t*.
- Cardiac Output: CO2 rebreathing as a method for estimating Cardiac Output (C.O.). Fick Method.
- Pulmonary Function Testing, Lung Volumes Measurement Vital Capacity (Spirometry) Residual Volumes with VacuMed system Residual Volume or Nitrogen Washout by Wilmore Method(3)
- Rehabilitation
9.2 Studies of Metabolism
This involves the measurement of VO2 and VCO2 at rest for the determination of :- Basal Metabolism (Basal Metabolic Rate) Research studies of metabolic and endocrine disorders, such as diabetes Effect of training on Basal Metabolic Rate and Heart Rate
- Resting Energy Expenditures (REE) which is useful for studies involving nutrition and also has important application in weight loss programs and studies of eating disorders. For example, is a subject in a weight loss program really reducing his/her calorie intake?
- Substrate Utilization
- Nutritional Assessment, effect of a fat vs. carbohydrate diet on RQ
- Testing of drugs affecting metabolism or weight control
See also Dr. Andrew's Corner
9.3 Occupational Applications
Exercise Stress (CPX) Testing is frequently used in professions that require high physical demands, such asFirefighters
Police
Military
Rescue & Disaster Response Teams
Miners
Steel Mill Workers
Divers
Professional Athletes
Pilots
CPX testing in such professions may be used for:
- Pre-employment screening
- Routine fitness assessment
- Disability assessment and documentation
- Rehabilitation assessment and documentation
9.4 Clinical Applications
- Diagnosis of causes of exercise limitation
- Responses of cardiopulmonary variables in patients with cardiovascular disease or pulmonary disease
RESPONSE TO EXERCISE IN CARDIAC OR PULMONARY DISEASE (5)*
| Variable | Cardiac Disease | Lung Disease |
|---|---|---|
| VO2 Peak | Decreased | Decreased |
| Anaerobic Threshold | Decreased | Low or Normal |
| Heart Rate Reserve | Decreased | Increased |
| Breathing Reserve | Normal or Increased | Decreased |
| O2 Pulse | Decreased | Normal or Low** |
| Exercise PaO2 | Normal | Normal or Decreased |
| Exercise P(A-a)O2 | Normal or High*** | Increased |
| Exercise VD/VT | Falls Normally | Fails to fall normally |
| ECG During Exercise | Abnormal | Normal |
3. Exercise-induced asthma
(See also Turboaire Challenger cold air generator)
4. Pre- and post-operative evaluation
5. Disability assessment Functional capacity testing (METs)
6. Assessment of supplemental O2 requirement Assessment of oxygen desaturation (SAO2) during exercise
7. Evaluation of level of fitness / exercise prescription
Occupational fitness assessment (e.g. police or firefighters) Pre-clearance for exercise/fitness/weight loss program
8. Evaluation of cardiac and/or pulmonary rehab
9. Evaluation of Metabolic Disorders
10. Evaluation of Muscular Disorders
11. Nutritional Assessment
12. Resting Energy Expenditure (REE)
13. Fick Cardiac Output Calculations
14. Cardiopulmonary Rehabilitation
15. Measurement of physiological dead space and determination of the VD/VT ratio (Requires the EtCO2 option).
10. What is measured during a CPX test?
1. Oxygen Uptake Response
VO2max: This is the gold standard to measure functional capacity of the cardiovascular system to transport oxygen.VO2max depends on the mode of exercise, the degree of training and the integrity of cardiovascular function.
It is usually reduced in any sort of cardiopulmonary disease. In most cases, except in athletes, the presence of a normal or elevated VO2max virtually ensures the absence of any major cardiovascular or pulmonary diseases.
VO2max is expressed in ml/kg of body weight and relates to exercise tolerance.
2. Haemodynamic Responses
The behavior of heart rate, systolic and diastolic pressures and cardiac output, during exercise provides insight into cardiovascular response.3. Ventilatory Responses
Changes in Minute ventilation (VE), Tidal Volume (TV) and breathing frequency (f) reflect the magnitude of ventilatory response to exercise. The pattern of increase in tidal volume and breathing frequency may provide information about certain pulmonary and circulatory disorders.4. Metabolic Response
This usually involves the measurement of VO2 and VCO2 at rest. Metabolism is affected be diet, exercise, disease, climate variations, etc.5. Electrocardiographic Response
This represents the main focus of conventional ECG Stress testing. It is useful in defining the presence or absence of exercise induced ischemias as well as the presence or absence of dysrhythmias.Clinical exercise testing requires monitoring of ECG and prompt termination of exercise testing is mandatory when a patient develops signs of distress, such as changes of PQRST pattern.
11. Other Publication
1. GUIDELINES FOR EXERCISE TESTING (4) A Report of the American College of Cardiology/American Heart Association Task Force on Assessment of cardiovascular Procedures (Subcommittee on Exercise Testing) Reprints: Mr. David J Feild, Assistant Executive Vice President, American College of Cardiology, 9111 Old Georgetown Road, Bethesda MD 20814
2. Books PRINCIPLES OF EXERCISE TESTING AND INTERPRETATION By Karlman Wasserman, MD, PhD., James E Hanson, MD., Darryl Y Sue, MD., Brian J Whipp, PhD., Richard Casaburi MD, UCLA Medical Center, 274 pp, illus., 1994, 2nd ed.
3. Books RESOURCE MANUAL FOR GUIDELINES FOR EXERCISE TESTING AND PRESCRIPTION Edited by the AMERICAN COLLEGE OF SPORTS MEDICINE, Indianapolis, IN. (64 Contributors) 580 pp, 205 illus., 1993
4. Books GUIDELINES FOR EXERCISE TESTING AND PRESCRIPTION, 4th ed. Edited by the AMERICAN COLLEGE OF SPORTS MEDICINE, Indianapolis, IN. 314 pp, paperback, 1991
5. Books EXERCISE PHYSIOLOGY LABORATORY MANUAL Basic principles of field and laboratory testing, includes forms for data collection and typical calculations. By Gene M Adams, California State University-Fullerton 304 pp, illus, wirecoil, 1993, 2nd ed.
6. Books EXERCISE PHYSIOLOGY Energy, Nutrition, And Human Performance William D McArdle PhD, Frank I Katch EdD and Victor L Katch EdD 853 pp, illustrations, 1991, Third Edition
7. Books EXERCISE IN HEALTH & DISEASE Evaluation & Prescription for Prevention and Rehabilitation, 2nd ed. By Michael L Pollock & Jack H Willmore, 754 pg, 367 illus, 1990
8. Books PRINCIPLES AND PRACTICE OF PULMONARY REHABILITATION Up-to-date info about diagnostic techniques & rehabilitation By Richard Casaburi MD PhD & Thomas L Petty MD. 510 pp, 190 illus, 1993
References:
(1) Huszczuk, A., B.J. Whipp, and K.Wasserman. A respiratory gas exchange simulator for routine calibration in metabolic studies. Eur. Respir. J. 3:465-468, 1990
(2) Gore, C.J., P.G. Catcheside, S.N. French, J.M. Bennett, and J. Laforgia. Automated VO2 max calibrator for open-circuit indirect calorimetry systems. Med. Sci. Sports Exerc 29:1095-1103, 1997
(3) Wilmore, J.A., P.A. Vodak, R.B. Parr, R.N. Girandola an J.E. Billing. Further simplification of a method for determination of residual lung volume. Medicine and Science in Sports and Exercise Vol. 12, No. 3.
(4) SPECIAL REPORT: Guidelines for Exercise Testing. JACC Vol. 8, No. 3. Sept 1986:725-38
(5) ACCP, San Francisco1991, A Pulmonary Approach to Exercise Testing, Idelle M. Weisman, FCCP, El Paso, TX
By Andrew Huszczuk Ph.D. (Application Note No. 17800-A1)
Why Calibrate Ergometers
All cycle ergometers are essentially machines that convert pedaling motion or arm cranking into rotation of a mass in the from of a flywheel, upon which a braking force can be applied. This conversion is practically always associated with an increase of the speed of flywheel rotation with respect to the cranking rotational rate by a factor of 4 to 30 depending on the number of gear-up stages or principle of speed transmission utilized. Consequently, the following factors determine accuracy and the long-term performance of cycle ergometers:
- Soundness of mechanical transmission determined by lubrication and storage conditions i.e. protection from corrosion and contamination by deposits of dust or other abrasive particles.
- Consistency of the braking force applied to the flywheel by a variety of physical means such as friction, electromagnetism etc.
- Accuracy of the braking force control from the point of view of temporal and thermal stability as well as utilization of feedback inputs such as temperature, torque and rotational speed.
All of the above factors can and usually do change the crucial performance parameters, although the resulting hindrance of the load setting accuracy may vary, usually from 5 to 20% of the intended one. Therefore, in research, diagnostic, health rehabilitation or even fitness training applications of cycle ergometry the correctness of the load setting and the pedaling cadence display becomes a matter of professional excellence, competence or neglect.
Some brands of cycle ergometers are equipped with simple means of periodic calibration, generally consisting of hanging known weights on a friction brake belt-tensioning gear or on a load cell torque feedback system. Still other, more advanced systems employ on-line monitoring and control of the transmission chain or belt tension as means of assuring the intended load setting. Although superior to no calibration at all, they do not and can not, however, verify the most important fact, namely, the amount of a rotational torque needed to be applied to the crankshaft to maintain rotation at any given cadence so that the amount of power expressed in Watts, Kilocalories/min etc. can be computed.
The most common causes of miscalibration appear to be:
- Electronic control system out of tune; this can affect the slope of the calibration curve as well as its parallel shift.
- Lack of maintenance, adverse storage or transport conditions or partial failure of bearing component usually shift the calibration curve upwards.
- Programming mistakes, usually involving internal or external software, EPROM's etc. are most difficult to detect without a dynamic calibrator as it does incorporate the "reassuring" static weight hanging calibration procedure yielding proper readings with improper programming or computational assumption.
The Cycloergometer Calibrator is designed to measure a rotational torque applied to a crankshaft in order to maintain a chosen R.P.M. while a variety of braking loads is imposed upon a flywheel of a cycle ergometer by frictional, electromagnetic or other controllable means furnished by a manufacturer. This calibration process is intended to verify manufacturer's claims as to the accuracy of load settings expressed in Watts. It can also verify the constancy of a given setting across a range of cadence expressed in R.P.M. in ergometers, which posses a research grade mode of operation called "isopower" or "hyperbolic". This mode, much preferred by exercise scientists, automatically controls the amount of braking torque to yield a work rate independent of cadence according to the formula:
Torque x Cadence = Watts x k = const.
or:
Kg*m x R.P.M./k = Watts = const.,
where k is derived as follows, if:
1W = 6.118 kg*m/min.,
then for a rotational movement:
Power = Torque x R.P.M./6.118/2pi,
so: k = 6.118/6.2832 = 0.9737
The source of rotary power consists of a D.C. motor and a worm-type speed reduction gear, rigidly mounted in a frame, which also hosts all additional electric and mechanical components of the apparatus. The output shaft of the reduction gear protrudes from one side of the frame in order to enable rigid coupling with the crankshaft of the cycle ergometer intended for calibration, whereas the input shaft is aligned and softly coupled with the shaft of the motor. The short rear end of this motor shaft holds the rotor of a tachometer, whereby the rotational speed (R.P.M.) can be measured and controlled.
The SCR type mains-powered motor speed controller allows adjustment of R.P.M. from 40 to 120 and regulation of the set R.P.M. regardless of the applied braking load.
The "S" beam load cell is mounted directly under the rear end of the motor. The whole load cell assembly can be either retracted into the underbelly of the calibrator for safety during transportation and storage, or locked in perpendicular position. In this perpendicular position it rests on the floor. A level adjuster is incorporated to position the calibrator horizontally using a water level as an indicator.
The control panel holds all the remaining electric and electronic components such as a load cell amplifier, an isolation amplifier with signal ratio circuits, a power supply, a panel LED display, adjustment potentiometers, fans, receptacles and switches.
The Calibration
Tools are included for removing the left crank of the ergometer. The user manual cautions that the cycle ergometer to be calibrated must be firmly secured in a steady position so that it cannot become unstable during calibration.
These are steps to follow:
- Place a cycle ergometer on a firm even floor. Avoid carpeting. Provide ample space for approaching it from its left side.
- Remove the left crank. (Detailed instructions are provided in the user manual).
- Install the shaft coupler and firmly tighten the nut or bolt that originally held the crank. Again, detailed instructions are provided.
- Insert the output shaft of the calibrator, with key and keyway aligned, into the coupler, thrust all the way in and tighten with the provided wrench. Level the calibrator as indicated by the water level.
To assure high accuracy of calibration, the calibrator itself needs to be briefly calibrated, which involves a few simple steps (detailed in the manual) that lead to the attachment of the provided calibration bar
Then:
Turn on the power switch and re-level the calibrator. Set the display selection switch to Watts or kg*m and adjust the reading to zero with the dial knob.
Hang a known weight (your own or the optional 5kg weight standard available from VacuMed) into the groove of the calibration bar. This groove has been machined at a distance of 66cm from the center of the output shaft, the resulting torque (using a 5kg calibration weight) can be computed as follows:<
Torque = 0.66 x 5 = 3.3 kg*m
which should appear on the display set to show torque values. If the reading differs from 3.30, adjust the trimpot labeled "CAL". Now, switch the display to Watts. It has been electronically ratioed to read Watts corresponding to a cadence of 60 RPM, which is widely regarded as a typical standard. The reading should reflect the following relationship:
Watts = Torque x 60/0.9737 = 3.3 x 60/0.9737 = 203 W
Remove the weight. Now the set-up is ready for calibration of the ergometer.
To ascertain the mechanical condition of the ergometer, begin calibration without turning its power on. Use the standard speed setting of 60 RPM as monitored by the panel meter, or via the output cable with your data acquisition system or just by an auxiliary voltmeter. (Instructions and calibration charts are in the user manual)
A typical power off, i.e. purely mechanical (frictional) wattage reading at 60 RPM is 10 - 20 W. If it reads more, your ergometer may need lubrication and cleaning. Now turn the power on and set the lowest available braking, which is usually from 25 to 30 Watts, as the lower settings are not reliable because of varying mechanical friction.
When setting different than 60 RPM cadence, derive actual Watts by multiplying the panel meter reading by the RPM/60 factor.
Example: Panel meter reads 100W at 90rpm,thus power = 100 * 90/60 = 150W
Proceed to higher settings at your preferred Watt increments. You may use the continuous ramp incrementation - a frequent experimental mode - to perform whole calibration by processing the data collected via the output cable and stored in your data acquisition system.
Conclusion
Ergometer calibration is essential in most research, clinical and fitness assessment settings, especially in applications such as:
- Multi-center study involving many cycle ergometers, often of different make, age and maintenance history. Any comparison or pooling of data will be greatly compromised by nonuniformity of true versus intended load settings.
- Health rehabilitation programs conducted in groups of patients with strictly prescribed exercise regimens requiring uniform performances of all available ergometers, whether "in house" or distributed to patient dwellings.
- High-end athletic performance testing in training centers specializing in specific conditions (e.g. high altitude, hyperbaric or climatic chambers etc.) where lack of an ergometer's calibration will hinder interpretation.
- Simple fitness tests required in military, police etc. to assess sustained qualifications for service. Often, rejected or disqualified individuals may challenge adverse decisions on the grounds of faulty measurement process.
Cycle ergometers are referred to as "ergometers", "stationary bicycles", or simply "bikes".
Your budget and the intended application determine the selection of an ergometer. Obviously, for home use you will expect to spend substantially less than for professional use, but even here it makes a difference whether the user is a fitness buff or a cardiac patient.
- Smoothness of ride
- Minimum braking (workload) resistance
- Maximum braking (workload) resistance
- How important is accuracy of the workload setting
- Is the set workload dependent or independent of pedaling speed
- Do you plan to interface the ergometer with a computer
- Do you need an integrated heart rate meter that will automatically keep the workload within your target heart rate zone
Upright vs. Recumbent Ergometer
Both versions are available for home or professional use. Upright ergometers are in predominant use, but people with severe exercise limitation, unsteady patients who might fall off an upright bike will be more secure on a recumbent bike.
Recumbent ergometers result in a lower blood pooling in the legs and groin discomfort is less of a problem, but most individuals reach lower VO2max in the recumbent position.
Home Use
Cheap ergometers are available for home use at discount stores for less than $100, but are they worth it? If you need a toy for the kids or you need to make a gift to someone you don't like - maybe. The problems are many: Flimsy construction, light flywheel, jerky braking, inaccurate and unstable workload. They just will not last and they are no fun to use. We know, exercise isn't always fun anyway, but if you are sitting on one of those cheap bikes and you are worried about breaking something, the ride is jerky, the power indicator unsteady; you will add stress instead of relieving it. And how will you know if you are improving, if the braking (workload) force is unstable or inaccurate? But, most importantly, insufficient flywheel energy necessitates more isometric effort (jerky pedaling) which causes higher elevation of blood pressure thus may be dangerous.
Plan on spending at least $ 600 for the model 17809 or $ 625 for the model EC3200. The maximum workload of the EC3200 is about 270 watts, enough to give a moderately fit person a good workout. About $1000 will buy an ergometer with workload that is independent of pedaling speed and capable of heart rate controlled exercise.
Professional Use
Professional use means use in a health club, doctor's office, rehab facility, fitness or sports training center, research or Olympic level training center.
A rehab facility may be interested in low minimum workload, since some patients may not be able to overcome the initial starting torque to get the pedals moving. So-called initial "zero-watt" ergometers have a motor that reduces this starting torque to almost zero. Accuracy is also important, otherwise it will be difficult to measure progress.
Fitness clubs are interested in sturdy, low maintenance work horses, not necessarily accuracy.
Athletic training centers will be more interested in maximum workload; we have models that go to 400, 800 or even 1200 watts. Accuracy here is important, a few watts will make the difference between winners and losers.
Professional or advanced bikers may want to mount their own bike on a stationary treadmill-like device, such as our number CS-1000 Cyclo-Simulator, or they will insist on being able to adjust the saddle and handlebar position in several directions, our model Excalibur Sport allows you to do this.
Wind-braked Ergometers
This is a special class of ergometers that use a fan-type wheel, where air resistance against the fan blades increase workload with the speed of pedaling.
These ergometers present a special calibration problem, as aerodynamic resistance will depend on room temperature, barometric pressure and air humidity.
Special Requirements
We can repair and calibrate most ergometers, or modify ergometers for pediatric use, just let us know your special requirements.
Breathing Reserve (BR) is usually determined during a pulmonary exercise stress test. It is the difference between the maximal voluntary ventilation (MVV) and the maximum ventilation measured during the exercise test.
Normal males have a breathing reserve of 15 liters per minute or 20 to 40% of the MVV. (Wasserman et al)
Some experts do not believe direct MVV measurement to be reliable because it is very effort dependent and is very difficult to put acceptability criteria together. However, FEV1 is well defined, when and how is it acceptable. Therefore, it is a fairly well-defined measure that can be used to predict the MVV.
The formula for MVV, when derived from FEV1 is 40 * FEV1 or some are using 35 * FEV1.
Calculation: BR (L/min) = MVV - Max VE.
BR% = (MVV - VE / MVV) x 100.
Example: If MVV = 82 L/min and
VE at max exercise is 65 L/min,
Then:
BR = 82 - 65 = 17
BR% = (82 - 65 / 82) x 100 = 21%
Last update: 11/1/08
By: Andrew Huszczuk and John Hoppe
There is no advantage to true BBB measurements, and in fact there are distinct disadvantages!
Early publications about measurement of VO2 and VCO2 date back to the early 1900's, with collection of exhaled gases in bags.
Then in the 1930's Douglas used gas collection bags during his expedition to the Andes; the resulting publicity credited him with the term "Douglas Bag". The collected gases were subsequently analyzed and their volume measured.
Douglas bag and mixing chambers measurements using discrete gas analyzers were the standard until computers made on-line measurements with mixing chambers relatively easy.
In the late 1960's, Beaver and Wasserman of Harbor-UCLA developed the first Breath-by-breath (BBB) measurement system and later with Brian Whipp became the gurus and advocates of BBB measurements. It was hoped that the intra-breath information of BBB measurements would yield information about the dynamics of muscle O2 uptake.
With the strong influence of the Harbor-UCLA team on purchasing decisions of new customers, many instrument manufacturers were eager to follow what was thought to be the future trend in VO2 measurements. However, the promise of measurement of muscle dynamics using BBB measurements failed totally.
Today, there is almost total consensus among experts in the field of VO2 measurements that there is not a single advantage to BBB measurements, and in fact definite disadvantages due to much more noisy data and unavoidable measurement errors at both very low and high ventilation rates*.
Copyright (C) 2008 Vacumetrics Inc
* See also "Breath-by-Breath (BBB) vs. "True Breath by Breath"
on VacuMed.com (Dr. Andrew's Corner)
5 June 2008
VO2 means oxygen consumption and usually refers to
the volume of oxygen consumed in 1 minute.
The following is written in the context of VO2 measurements for fitness or athletic evaluation. Clinical VO2 testing most often involves the monitoring of EKG and other physiologic indices,
and the reason for the test most likely will be to assist in diagnosis of disease or measurement
of disability or progress of rehabilitation.
The air we breathe contains roughly 21% oxygen (O2), 78% Nitrogen (N2) and various trace gases, such as Argon, Carbon Dioxide (CO2) and a few more.
We can ignore N2 in our discussion, since it does not partake in metabolism.
-
- Note: Wondering why the "2" as in O2 and CO2? Perhaps you had the measles when this subject was discussed in school. The reason
-
- is that some gas molecules get lonesome and always hang around in pairs.
- Of course, your chemistry teacher would have a more elegant explanation, but would we Dummies understand it?
So we inhale 21% O2 and exhale, typically, 17%O2 and about 4% CO2. We have consumed, "burnt", metabolized roughly 4% oxygen. Of course, nothing is ever that simple, because the first part of your exhalation is the very last part of your inhalation. So it is still nearly 21% O2, but then as the source of exhaled gas comes from deeper in the lungs, it contains more and more CO2, and less and less O2. This change in gas concentration occurs rapidly, and the precise measurement requires some sophisticated instruments.
Much easier to measure are mixed exhaled gases. Assume you exhale into a plastic bag, close the bag quickly and massage it so that you are sure the gases are mixed. Now a single measurement of this mixture will give you mixed exhaled O2 and CO2, again, ignoring N2. As I said above, the typical mixture will contain from 16% to 17% O2 and 3% to 4% CO2. That in itself tells us only that we are alive, it does not tell us how much O2 we consumed. For that we need to know or measure the volume of the bag. Exhaled volume is mostly expressed as "VE" (Volume, exhaled) or "minute ventilation". You guessed it, it means the volume exhaled in 1 minute.
In practice, we want to measure not just one breath, but the gas concentrations and volumes of many breaths over longer time periods. This early method of gas collection in large bags, known as the "Douglas Bag Method", is still practiced by some purists and for teaching purposes, but modern, computerized instruments greatly simplify those measurements. Computers also take care of necessary corrections for temperature, humidity and barometric pressure.
Now to calculate VO2, a simplified equation might look like this:
- VO2 = VE x (O2inspired - O2expired)
In plain language, this means VO2 equals the total volume of gas exhaled in 1 minute (VE) multiplied by the difference between inhaled and exhaled oxygen.
So if you exhaled a total of 10 liters of gas during 1 minute, and your mixed exhaled O2 is measured at 17%, then
- VO2 = 10 x (0.21 - 0.17)
(Note that 21% and 17% must be written as a fraction,
which is 0.21 and 0.17)
- simplified to: VO2 = 10 x 0.04 = 0.4
so your VO2 in this example would be 0.400 liters (or 400 milliliters) per minute, which is close to typical for a person at rest.
But that is usually not the end of the calculation. Surely, it is obvious that the VO2 of a mouse will be so much less than that of a human. Just the same, the basic VO2 of a small person will be less than that of a much larger person. It is conceivable, therefore, that a maximum oxygen consumption (VO2max) of 2 liters of a 5 foot tall person may actually make him or her more fit that the VO2max of 2.5 liters of a 6 foot tall person.
How do we take care of that?
Well, we report VO2 in relation to body weight in kilogram. For this calculation liters are converted to milliliters by multiplying liters x 1000.
-
- Example: The 5-footer has a body weight of 60kg, so her VO2max of 2 liters divided by her body weight equals to 33 milliliters per kg (ml/kg). (2000 divided by 60)
The 6-footer weighs 90kg, so 2500 divided by 90 = 27.7 milliliters per kg.
You see, the 5-footer really has a higher VO2max when expressed in milliliters per kilogram of body weight. It's not only fair, there is just no other way to compare the mouse to the elephant (or the human).
Naturally, all this is still a bit of oversimplification, but good enough for us Dummies.
To continue to chapter 2, click here:
Why measure VO2
Copyright (C) John Hoppe 2008
12-12-08
Why measure VO2 ?
You take a 15-minute walk during your lunch hour, are you fit? Your neighbor plays golf twice a week, is he fit? Your mother tends her garden every day, is she fit? Your cousin runs a marathon several times a year, is she fit? (Oh yah) Who is fit? Who is not?
VO2 measurements are useful in a number of applications. There is the Resting VO2 test, the sub-maximal and the VO2max.
Resting VO2 is always expressed in ml/kg. You see terms like REE (Resting Energy Expenditure), RMR (Resting Metabolic Rate) and BMR (Basal Metabolic Rate). The differences are subtle, depending how you prepared for the test.
Most resting VO2 tests, as a person in a fitness facility might experience, involves refraining from exercise, food and stimulating liquids for a few hours, then getting comfortable in a reclining position and finally breathing into a face mask for several minutes in order to analyze your exhaled breaths.
Your REE or RMR is that O2 required to sustain your basic body function without any voluntary or involuntary (such as shivering) muscle movement. With that information, conclusions may be drawn about your dietary needs; about weight loss management, and adherence to a weight reduction program may be monitored. More on www.vacumed.com, click on "Dr. Andrew's Corner".
VO2max testing typically involves a graded exercise test, meaning the workload is steadily increased to exhaustion. In a sub-maximal test workload is usually increased to a pre-determined heart rate or workload short of a maximal effort, or to a point that determines the lactate or anaerobic threshold (next chapter). Formulas have been published to predict VO2max from a sub-maximal test, but there are considerable doubts about the accuracy of such predictions.
A poor analogy might be to claim that you could predict the maximum speed of a car by accelerating to 55 miles per hour.
VO2max (Maximal oxygen uptake) was first described by Hill and Lupton in 1923 as "the oxygen intake during an exercise intensity at which actual oxygen intake reaches a maximum beyond which no increase in effort can raise it".(1) In other words, there is a point at maximal exercise where your oxygen consumption no longer increases, even though your workload does increase further. To be sure, you can perform this supra-maximal effort for a very limited time, typically less than a minute.
VO2max can be considered THE universal measure of aerobic fitness. It allows you to compare couch potatoes with runners, rowers with tennis players, swimmers with spinners, and so many more. It does not tell you about their skill, just their relative ability to perform work. Let's look at two runners, equal in weight. Runner #1 has a maximum VO2 (VO2max) of 3 liters, runner #2 a VO2max of 3.3 liters. Yet runner #1 beats runner #2. This may be because runner # 1 has better skills, running efficiency, Nike shoes, or better steroids. But it could also mean that if runner #2 improved his skills, he has the potential to be the better runner.
Modern, computerized VO2 measurement systems will compare your test results with "predicted" or so-called "normal" values. Such normal values have been published in the literature and are based on testing groups of "typical" populations, broken down by gender, age, height, and in some cases, ethnicity. A typical printout of such a VO2max test is shown below.
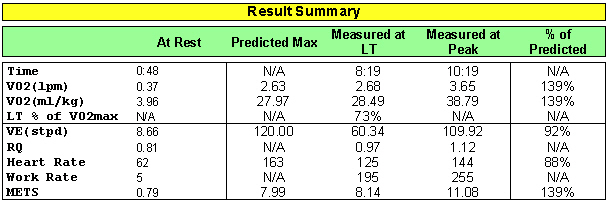
Figure courtesy of VacuMed
Between resting and maximum VO2 measurements are the "Thresholds": Ventilatory, lactate, anaerobic. We will talk about this in a future chapter.
In medicine, there are additional reasons for measuring VO2, but this may get too complicated for us Dummies.
Click here to see a video of a typical VO2 test
Click here for more
Sample Printouts
To continue to chapter 3, click here:
Anaerobic, Lactate and Ventilatory Thresholds
(1) Hill, A. V. and H. Lupton, Muscular exercise, lactic acid, and the supply and utilization of oxygen. Q. J. Med. 16:135-171, 1923
Copyright (C) John Hoppe 2008
12-27-08
All references to thresholds here are in relation to VO2 testing. A search of the literature, or Google, will find references to other methods of determining some thresholds. But beware, there is much mis-information on the web!
For the Aerobic Threshold I found this explanation in Wikipedia(1):
"The aerobic threshold (AeT) is a term sometimes used by sports coaches and trainers to describe a level of exercise intensity somewhat below the anaerobic threshold. It, however, is not a defined physiological term.
The AeT is sometimes defined as the exercise intensity at which blood lactate reaches a concentration of 2 mmol/liter (at rest it is around 1 mmol/liter). This tends to be at a heart rate of approximately 20-40 bpm less than the anaerobic threshold."
In physiology, AeT refers to an increase in ventilation (breathing volume) that occurs rather early in an exercise session, sometimes also called the first ventilatory threshold (VT1).
The Lactate Threshold (LT): Blood lactic acid increases with increasing exercise workload. Most lactic acid is re-cycled in the muscles and liver, a very complex process. Every individual has a point (work rate) where the rate of lactate production exceeds the rate of re-utilization. At that point the lactic acid then increases disproportionately to workload. This point is called the lactate threshold. To determine this point it is necessary to puncture (lance) your skin (typically earlobe or fingertip) every 1 to 2 minutes and collect a drop of blood for analysis.
The Ventilatory Threshold (VT or VT2). At the LT, or very close to it, your ventilation also increases disproportionately to increases in workload. When plotted on a graph, this is often the most recognizable event demarcating the ventilatory threshold, see figure 1. When workload increases at a steady, linear rate, and ventilation initially follows with a like increase, then a sudden deviation is certainly an event that must have significance.
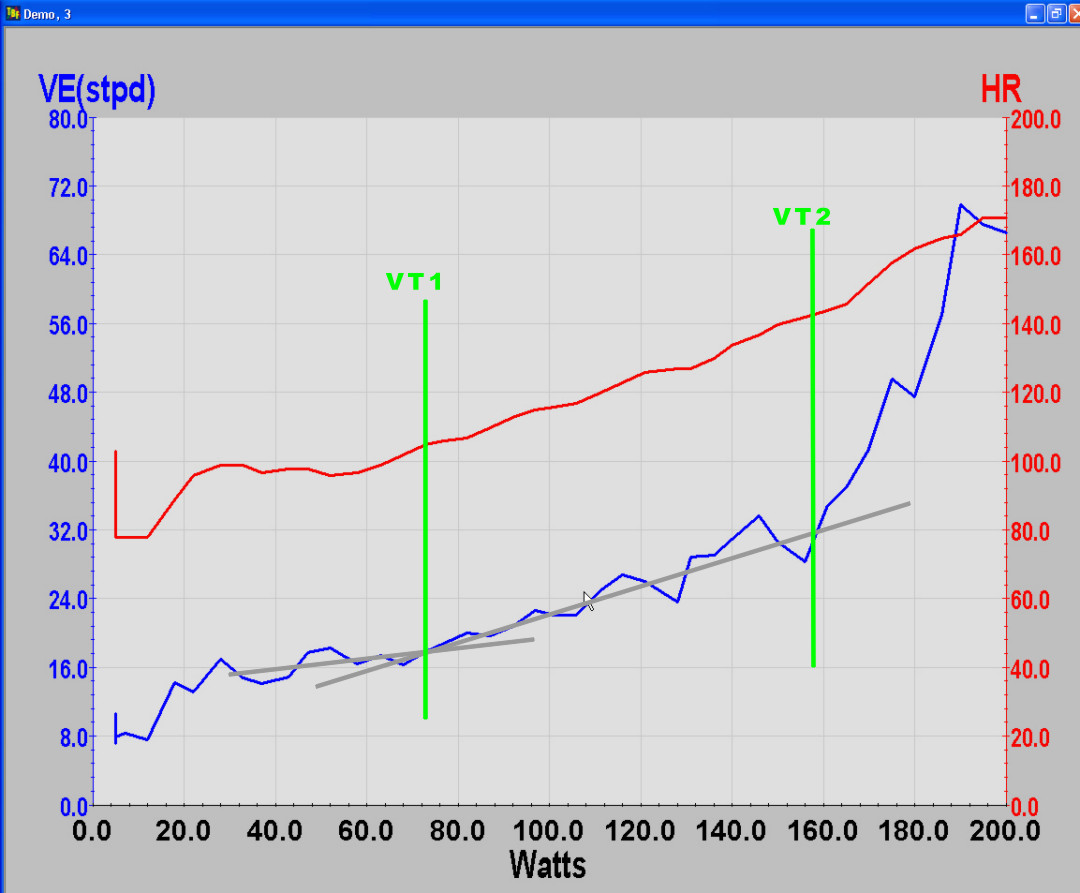
Figure 1
Figure 1 shows Ventilation and heart rate plotted against a linear
increase in workload. VT1 and VT2 are determined by changes in slope of ventilation.
The Anaerobic Threshold (AT). "Anaerobic" means "without air" and now we are stepping on thin ice. The term "AT" was originally suggested by Dr. Karlman Wasserman of UCLA, but the term and the scientific reasoning behind it have been seriously questioned in recent years. It's safe to say that the AT is going out of favor.
Ok, there is agreement that there is a threshold "T", a change in physiologic response to increasing workload, an unbalance. Scientists are still debating the cause. The issue is what to call it. Some have called it the Fitness Threshold, Thermal Threshold etc. The most important point here is that, for most people and under most conditions, the LT, VT and AT occur at the same point, although nit-picking scientists will quibble and split hairs that us Dummies either can't understand or don't care about.
There is also agreement that you can perform work for prolonged periods below the "T", but working above the T will quickly lead to exhaustion.
There is further growing consensus that the T measurement may be more useful than VO2max for most people. After all, unless you are a super athlete that wants to brag, or may otherwise benefit from knowing your VO2max, what's the point? The fact is, VO2max test results depend very much on motivation. Is a person that is trying to collect disability payments motivated to perform well?
The "T" clearly defines the limit of your day-to-day operational capability. For untrained individuals, the T may be approximately 50% of their VO2max, for trained athletes it will be more like 80 to 90% of their VO2max, therefore, the T is either expressed as a percentage of VO2max, or in liters of VO2 per minute, or as the heart rate at the T for training purposes. Nevertheless, this suggests valuable implications for athletic training, where the goal is to move the athlete's T as close to VO2max as possible.
Since the T is less dependent on motivation, and does not require exercising to exhaustion, it can be measured more often for a person engaged in a fitness program. Increasing your T is what you should aim for and even us Dummies know that frequent exercise of most any kind will get you there.
(1) Wikipedia is a registered trademark of the non-profit Wikimedia Foundation
Copyright (C) John Hoppe 2008
12-12-08
Most University testing for athletic purposes only. Prior appointments are necessary!
1.
Dr. Desmond Ebanks
Alternity Healthcare LLC
639 Park Road
West Hartford CT 06107
Tel: 806-748-4064
Click here for Alternity Healthcare web site
2.
Dr. Marc Silberman
NJ Sports Medicine & Performance Center
689 Valley Road
Gillette NJ 07933
Tel: 908-647-06464
New Jersey Sports Med web site
3.Mike Craven
Mechanicsville Fitness Center
aka: Mike's Olympic Gym
7495 Old Hickory Drive
Mechanicsville VA 23111
Tel: 804-543-9293
3.A
Chris Eschbach, PhD
Meredith College
Raleigh, No Carolina
Lab phone: 919-760-8769
Meredith College VO2 testing web site
4.
Out of business, but link still active:
Click here for G2 Health web site
5.
Ohio University
Work Physiology Laboratory
001 Irvine Hall
Athens OH 45701
Tel: (740) 593-2291
FAX: (740) 797 2778
e-mail: hagermaf@ohio.edu
6.
Nathan "Nate" Thomas
Mobile Utah Testing Lab
Salt Lake City UT
Tel: 801-302-9549
FAX: 801-397-2118
Nate@hakenya.com
Hakenya web site
7.
University of Las Vegas
Exercise Physiology Lab
Box 53034 Kinesiology Dept
4505 Mryland Pkwy
Las Vegas NV 89154-3034
Tel: (702) 895-3766
FAX: (702) 895-4191
e-mail: lagolding@aol.com
8.
Ken Nicodemus
Exercise Physiologist / Director
The Fit Stop Human Performance Lab
Tel: (760) 634-5169 Fax: (866) 409-5888
Fit Stop web site
9.
Holden MacRae
Pepperdine University
Dept of Sports Medicine
Malibu CA
Tel: (310) 456-4278
FAX: (310) 317-7270
e-mail: holden.macrae@pepperdine.edu
10.
Susan Ceriale
Wellness & Fitness Institute
University of Santa Barbara
Santa Barbara CA 93106
Tel: (805) 893-4000
FAX: (805) 893-7054
e-mail: sceriale@gte.net
11.
Steve DaMassa
Clark Community College
Fitness Testing Lab
1933 Fort Vancouver Way
Vancouver WA 98663
Tel: 360-992-2185
e-mail: sdamassa@clark.edu
12.
Cheryl Pitkin
Central Oregon Community College
Exercise Physiology Lab
2600 NW College Way
Bend OR 97701
Tel: (541) 383-7768
Click here for COCC web site
13.
L. Brilla
Western Washington University
MS-9067
Bellingham WA 98225
Tel: (360) 2861
e-mail: physlab@cc.wwu.edu
14.
Brendan Roach
BodyLab Ltd.
43 Hania St
Wellington, New Zealand
Tel: +644-801-17395
Click here for BodyLab web site
Click on U-tube icon for video
15.
Dr. Marcus Strozberg
Meduna do Esporte
2. Osvaldo, S912
Brasil
Tel: +55-85-266-4132
e-mail: strozberg@secrel.com.br
Resting Energy Expenditure "REE"
©1998 VacuMed
By Denise Schwartz, MS, RD, FADA, CNSD
What does REE mean?
Resting energy expenditure represents the amount of calories required
for a 24-hour period by the body during a non-active period. Energy
expenditure can be estimated by numerous published formulas. There are
nearly 200 published energy expenditure formulas dealing with various
conditions, disease states, age, presence of obesity and other
additional factors. (5) One of the most frequently used formulas for
predicted energy expenditure are the Harris-Benedict equations. These
were established in 1919 and took into account gender, age, height and
weight. However, these formulas are skewed towards young and non-obese
persons. (2)
Harris-Benedict Equations (calories/day):
Male: (66.5 + 13.8 X weight) + (5.0 X height) - (6.8 X age)
Female: (665.1 + 9.6 X weight) + (1.8 X height) - (4.7 X age)
weight in kilograms, height in centimeters, age in years
The Harris-Benedict equations have been found to overestimate by 6% to
15% the actual energy expenditure measurements done by indirect
calorimetry. (3) There is a large variation between individuals, when
comparing their measured energy expenditure to the calculated amount.
These equations have limited clinical value when tailoring nutrition
programs for specific individuals for weight loss purposes or acute as
well as chronic illness feeding regimens.
Energy expenditure can be measured directly by putting a person in a
calorimeter and measuring the amount of heat produced by the body mass.
This is expensive and very impractical in the clinical setting. Energy
expenditure can be measured indirectly with a metabolic cart by
analysis of respired gases (usually expired) to derive volume of air
passing through the lungs, the amount of oxygen extracted from it
(i.e., oxygen uptake VO2) and the amount of carbon dioxide,
as a by-product of metabolism, expelled to atmosphere (CO2 output – VCO2)
– all computed to represent values corresponding to 1 minute time intervals.
With these measurements the resting energy expenditure (REE) and respiratory quotient (RQ) can be calculated.
The RQ represents the ratio of carbon dioxide exhaled to
the amount of oxygen consumed by the individual. RQ is useful in
interpreting the results of the REE. The abbreviated Weir equation is
used to calculate the 24-hour energy expenditure. These measurements
are printed out by the metabolic cart after completion of the indirect
calorimetry test. (1,4,5)
Abbreviated Weir Equation:
REE = [3.9 (VO2) + 1.1 (VCO2)] 1.44
VO2 = oxygen uptake (ml/min)
VCO2 = carbon dioxide output (ml/min)
Respiratory quotient (RQ) = VCO2/VO2
Benefits of using REE in the clinical setting
The REE is useful to prevent under and overfeeding of individuals,
especially in the acute care hospital setting. Excessive calories or inadequate feeding regimens can have detrimental effects on clinical outcomes of patients' care. Malnutrition can result from feeding a patient less than his/her metabolic requirements leading to reduced respiratory muscle strength, increased risk of infection, poor wound healing and impaired normal body function. Overfeeding means providing too many calories that can not be used by the body and are therefore converted to fat storage.
This can cause more CO2 to be produced and result in increased work of breathing. The REE measurement is especially beneficial in the ventilator dependent patient population during the process of weaning
the individual from mechanical ventilation to resume (reestablish) spontaneous breathing. (7)
How do you do the test?
For best results, when having a REE done, there are certain conditions
that need to be controlled and others that just require documenting
at the time of the test. During the test the individual is interfaced with a
metabolic measurement system by means of a facemask or a canopy.
A mouthpiece with a nose clip is also sometimes used, but it may create
overly stressful conditions to a subject (patient).
Important considerations or conditions to improve the REE measurement:
(1,4,5)
Individual should rest for at least 30 minutes in bed or a
recliner before the test, however, the person should not be asleep.
No food for at least 2 hours before the test.
Maintain quiet surroundings when the test is in progress and normal temperature. The individual should not move arms or legs during the test.
Normal room temperature should be maintained, avoid drafts or any condition that might result in shivering.
Medications taken should be noted, such as stimulants or
depressants.
Steady state should be achieved, which would be identified
clinically by the following:
5 minute period when average minute VO2 and VCO2
changes by less than 10% and the average RQ changes
by less than 5%.
Stable interpretable measurements should be obtained in a 15 to 20
minute test.
Additional considerations for hospitalized individuals:
If the individual is on specialized nutrition support (enteral or
parenteral nutrition) continuous 24-hour infusion does not need
to be stopped. The nutrients infused should be constant for at
least 12 hours. If feedings are intermittent or cyclic, the feeding
should be held for at least 2 hours. Document the product and
the rate the individual is receiving.
Discontinue any supplemental sources of oxygen if the individual is on room air, which includes nasal cannulas, masks or tracheostomy collars.
If the individual is on a ventilator, the settings should remain
constant for at least 1-1/2 hours before the test.
No recent chest therapy or physical procedures.
Renal failure patients requiring hemodialysis should
not be tested during dialysis therapy.
Interpreting the REE
Interpreting the measured REE includes comparing the results to the
predicted level of energy needs for that individual. Determining the 24
hour calorie intake of that individual from either an oral diet or
specialized nutrition therapies (through feeding tubes into the
gastrointestinal tract or intravenous administration) is required.
It is important to assess the RQ to make certain it is within
physiological range and consistent with the person's calorie intake
and medical history. The physiological range of RQ is 0.67 to 1.3. This value
represents the combination of carbohydrate, fat and protein being used
for energy. If the RQ is greater than 1.0, decrease the total calorie
intake and adjust the carbohydrate to fat ratio. If the RQ is less
than .81 increase the total calorie intake, dependent on the goal for
the nutrition therapy. Food sources and conditions have specific RQ
values that are useful when interpreting the REE and making
recommendations for changing dietary goals and feeding regimens. (1,4,5)
Energy source/condition RQ
prolonged ketosis <0.70
fat 0.70
underfeeding <0.71 protein 0.80 mixed energy 0.85 carbohydrate 1.00 fat storage >1.00
Use of REE in conjunction with weight management programs
In weight management programs, when an individual has trouble losing
weight a frequent comment is that ones metabolism is slow. This can
result in failure of the individual to adhere to a weight management
program incorporating a reduction in total daily calorie intake.
However, once the actual REE is done, there is no longer need
to speculate about the normalcy of metabolism for that person.
Successful maintainers of weight loss report continued consumption of a
low-energy and low-fat diet. (8) Efforts to improve weight loss and
maintenance need to focus on strategies to increase calorie expenditure
through exercise and an appropriate diet based on measured energy needs.
The goal is a lifelong commitment to healthful lifestyle behaviors. (6)
An example of how to successfully use the REE measurement in a weight
management program requires interpretation and counseling by a
registered dietitian. After measuring the REE and calculating the 24
hour intake, the individual would be instructed on reducing their food
consumption by approximately 200-300 calories a day below the
measured REE. This should result in about 1 pound weight loss per week
with additional weight loss due to exercise. If the REE is extremely
low then the focus would be on maintaining the calorie intake at the REE
level and gradually increasing to at least 30 minutes of enjoyable
activity each day.
Clinicians monitoring weight management programs would be able
to determine if their clients are actually following a reduced calorie
diet based on REE, RQ and the amount of weight loss. These
measurements would be very useful in detecting failure to adhere
to the diet and facilitate better understanding by the client in
achieving his/her weight goal.
It is important that an individual have a framework for making healthful
food choices to obtain realistic weight reduction and maintenance
goals. The challenge is to balance adequate nutrient intake with the
individual's desire to lose weight rapidly and to address the numerous
myths concerning diet modification. The REE takes the guesswork out of
determining the goal for the calorie intake to achieve the desired
outcome.
References
1. Feurer I and Mullen JL. Beside measurement of resting energy
expenditure and respiratory quotient via indirect calorimetry. Nutr
Clin Prac. February 1986;1:43-49.
2. Frankenfield DC, et al. The Harris-Benedict studies of human basal
metabolism: history and limitations. J Am Diet Assoc. 1998;98:439-445.
3. Garrel DR, et al. Should we still use the Harris and Benedict
equations? Nutr Clin Prac. June 1996;11:99-103.
4. Matarese L. Indirect calorimetry: technical aspect. J Am Diet
Assoc. 1997;97(suppl 2):S154-S160.
5. McClave SA and Snider HL. Use of indirect calorimetry in clinical
nutrition. Nutr Clin Prac. October 1992;7:207-221.
6. Position of The American Dietetic Association: weight management. J
Am Diet Assoc. 1997:97:71-74.
7. Schwartz DB: Pulmonary failure. IN Matarese LE and Gottschlich MM:
Contemporary Nutrition Support Practice. Philadelphia, W. B. Saunders,
Co. (In press)
8. Shick SM, et al. Persons successful at long-term weight loss and
maintenance continue to consume a low-energy, low-fat diet. J Am Diet
Assoc. 1998;98:408-413.
The Metabolic (Lung) Simulator
Calibration of Metabolic Systems
Stress Testing
Resting Energy Expenditure "REE"
Why Calibrate Ergometers
How to select a Cycle Erometer
Deception of the Douglas Bag
a "met" was derived from the resting oxygen consumption (VO2) for a 70kg, 40-year-old male and its value is 3.5 ml/min per kilogram of body weight. Therefore, a person working at 5 mets would have a VO2 of 17.5 ml/min/kg.
Some laboratories estimate maximum METS from the maximum work rate achieved using the "Bruce" protocol without actually measuring VO2, which may lead to inaccurate results.
The History of (true) Breath-by-Breath Measurements
5 June 2008
By: Andrew Huszczuk and John Hoppe
There is no advantage to true BBB measurements, and in fact there are distinct disadvantages!
Early publications about measurement of VO2 and VCO2 date back to the early 1900's, with collection of exhaled gases in bags.
Then in the 1930's Douglas used gas collection bags during his expedition to the Andes; the resulting publicity credited him with the term "Douglas Bag". The collected gases were subsequently analyzed and their volume measured.
Douglas bag and mixing chambers measurements using discrete gas analyzers were the standard until computers made on-line measurements with mixing chambers relatively easy.
In the late 1960's, Beaver and Wasserman of Harbor-UCLA developed the first Breath-by-breath (BBB) measurement system and later with Brian Whipp became the gurus and advocates of BBB measurements. It was hoped that the intra-breath information of BBB measurements would yield information about the dynamics of muscle O2 uptake.
With the strong influence of the Harbor-UCLA team on purchasing decisions of new customers, many instrument manufacturers were eager to follow what was thought to be the future trend in VO2 measurements. However, the promise of measurement of muscle dynamics using BBB measurements failed totally.
Today, there is almost total consensus among experts in the field of VO2 measurements that there is not a single advantage to BBB measurements, and in fact definite disadvantages due to much more noisy data and unavoidable measurement errors at both very low and high ventilation rates*.
Copyright (C) 2008 Vacumetrics Inc
* See also "Breath-by-Breath (BBB) vs. "True Breath by Breath"
on VacuMed.com (Dr. Andrew's Corner)
5 June 2008
Here is what you need to measure VO2 via the "Douglas Bag Method"
You should also read Deceptions of the Douglas Bag Validation Method
in Dr. Andrew's Corner.
(Click on photo to enlarge it, then on BACK button to return)
The following components are required:
- Gas Analyzers
O2 Analyzer: See our 17620 , 17625 or 17518
CO2 Analyzer: See our 17630 or 17515
If you are using brand "X" gas analyzer you may also need our model 17503 Pump/Flow Controller, our own gas analyzers have a built-in pump.If you need a drying column for your gas analyzer Click here
- How to measure volume:
a. Dry Gas Meter # 17150
b. Model 17125 or 17130 Turbine Volume Meter, the best choice because it may later be incorported into a computerized metabolic measurement system, or
c. A Calibration Syringe to evacuate the gas collection bag in measured increments. We suggest the 7-liter size because if you test an athlete with 120 liter minute ventilation and you have a 1-liter syringe, it will take 120 strokes to evacuate the bag. Think about it!
If you choose the syringe method you will need the stopcock in (4) below. - A Patient Interface
Choose a mouthpiece , noseclip and breathing valve or
a more comfortable Air Cushion Mask.If you choose a mouthpiece and noseclip, we suggest you use the R2700B valve with saliva trap and either the R2726 or R2766 Head Support.
If you choose a face mask, we suggest you use the R2700 valve with the number KM295A mask starter kit.
- Gas Collection bags and related accessories
This usually means so-called "Douglas Bags", we suggest the 200 liter size for use in exercise. Each bag will need a number K-5311 closing valve.
To prevent damage to the bag, they should be suspended. Either rig a suspension wire in your lab or consider our number 1195-R Suspension Rack. Each rack can hold 3 filled bags.In addition to the closing valve, you need a manual stopcock. We suggest number R2100C. The purpose of the stopcock is two-fold:
a. To switch the test subject from exhaling into air to exhaling into the bag on command, and
b. To connect the evacuation syringe alternately to the bag and to air. - Barometric Pressure, Humidity & Temperature.
Required for BTPS, ATPD, ATPS and STPD corrections.
(We have the formulas if you need them)
Wasserman, Hansen, Sue & Whipp state: We believe the AT to be the best determinant available to demarcate the upper limit of work rate which can be endured for a prolonged period. Thus, a task performed below the AT can be sustained. A task performed above the AT cannot be sustained as long; the higher the work rate above AT, the less is its tolerable duration.
Also: The VO2 at which blood lactate level begins to be elevated has been used to define the AT in normal subjects.
In other words, the "AT" occurs at the same time as the Lactate Threshold "LT"
Body Fat
Analyzers
Biolectric Impedence Analysis (BIA)
BODYSTAT Body Composition Measurement Locations
1.
M-Dietician
Los Angeles,CA
Dr. Amy Lee, M.D.
(213) 977-1030 amylee@mdietician.com
2.
Next Level Fitness
Palm Desert, CA
Casey Washack
(760) 341-8200 nlf@nextlevelfitness.org>
3.
Palm Desert Athletic Club/Desert Fitness Group
Palm Desert, CA
Leslie Shuffleton, DFG
(760) 641-1550 leslie@desertfitnessgroup.com
4.
re:Form FITNESS Studio
San Marcos, CA
TK Smith
(760) 593-7512 tk@hereswhatido.com
5.
Brandon Weight Loss
Brandon, FL
Abida Saleh
(813) 684-5880 abida@shifa-llc.com
6.
Valdosta State University,
College of Nursing
Valdosta, GA
Dr. Melissa Benton or Dr. Maura Schlairet
(229) 245-3775-Benton or (229) 333-7192-Schlairet mjbenton@valdosta.edu or mcschlai@valdosta.edu
7.
Vital Life Health
Clarendon Hills, IL
Dr. Stephen Spates
(630) 734-3454 info@drspates.com
8.
Northshore Sleep Medicine
Skokie/Evanston, Il
Dr. Lisa Shives, M.D.
(847) 674-3600 lshives@nssleep.com
9.
University of Kentucky
Body Composition Core Laboratory
Lexington, KY
Jody L. Clasey, PhD, FACSM
(859) 257-8055 jlclas0@uky.edu
10.
Carrington Health Center
Wellness & Disease Management Department
Carrington, ND
Ryan Zink
(701) 652-7250 or (701) 652-3141 ryanzink@catholichealth.net
11.
Integrative Medical Center
for Wellness and Weight Management
New York, NY
Dr. Samoon Ahmad, M.D.
(212) 585-1111 samoon.ahmad@nyumc.org
12.
Dr. Howard Goodman D.C.
New York, NY
(212) 346-2030 goodmanhoward@yahoo.com
13.
Michelle Ross Nutrition
Michelle Ross, RD
Lodi, CA
(916) 253-3406 info@michellerossnutrition.com
=================================================
Hydrostatic Weighing (Under Water Weighing)Locations
Prior appointments may be necessary!
1.
Frederick C. Hagerman, Ph.D.
Ohio University
Work Physiology Laboratory
Athens OH 45701
Tel: (740) 593-2291
FAX: (740) 797 2778
e-mail: hagermaf@ohio.edu
Hydrostatic Weighing, DEXA, BodPod available
2.
Lawrence A. Golding Ph.D.
University of Las Vegas
Exercise Physiology Lab, Kinesiology Dept
Las Vegas NV 89154-3034
Tel: (702) 895-3766
FAX: (702) 895-4191
e-mail: lagolding@aol.com
BIA, Hydrostatic Weighing, DEXA, Calipers and BodPod available
3.
Wellness & Fitness Institute
University of Santa Barbara
Santa Barbara CA 93106
Tel: (805) 893-4000
FAX: (805) 893-7054
BIA and Calipers(5-points)available
5.
Johanna Olson
Central Oregon Community College
Exercise Physiology Lab
Bend OR 97701
Tel: (541) 383-7768
Click here for COCC web site
email: jolson1@cocc.edu
Hydrostatic Weighing available
Hydrostatic Weighing Tanks
"Bodystat 1500" Body Fat Analyzer
"QuadScan" Multi Freqency Body Composition Analyzer
"Lange" Skinfold Caliper
"Bodystat 1500MDD" Body Composition Analyzer
Software for Hydrostatic Weight Measurements
"SlimLAB" and "SlimLAB PRO" VO2 Measurement Systems for BMR/REE
Residual Volume Measurement System (RV, FRC, TLV)
Medical Body Composition Analyzer
"Harpenden" Skinfold Caliper: The Gold Standard of Calipers

Click here to calculate your monthly income: Body Fat Income Calculator
For a very useful tutorial on the various method of Body Composition Measurement methods Click Here
Click here for more Fitness Products
This is not a scientific review but rather a brief explanation of measurement techniques and a listing of products available from VacuMed.
Hydrostatic (or underwater) measurements are considered the "Gold Standard" of body fat measurements. Body fat measurements are an important factor in diet and exercise prescription.
Normal range of body fat percentage varies by sex, age and may be influenced by body build, here are some typical values:
Males to age 30 = 8 to 14%, females = 18 to 25%
Males at age 50 = 8 to 17%, females = 18 to 26%
Others have defined normal values for males 12 to 18%,
females 18 to 26%,
Some say the goal for males should be between 12 and 15%,
for females 18 to 22%.
Bio-Impedance Measurements
These electronic body fat analyzers send a minute current through the body and measures the resistance (impedance). When used properly, results are relatively accurate and repeatable. Results are displayed directly in % body fat, so no calculation is required.
More about the accuracy of low-cost Bio-Impedance Devices
Everyone wants to know about accuracy of these devices. The best and most accurate devices use electrodes that are pasted on a hand and a foot. Then there are integrated weighing scales, where the current is passed through the lower body only from one foot to the other. Some hand-held devices pass current through the upper body only from one hand to the other. So you can see that depending on where a person carries the most fat tissue, the various measurement techniques will produce different readings. But we maintain this: What does it matter if your body fat is 27% or 35%. If you are in a fitness program or weight reduction program, what matters is, is my body fat decreasing?
Skin Fold Measurements
This method utilizes a "Skin fold Caliper" to pinch the skin at several predetermined sites and measure the thickness of that pinch. The results are then summarized and evaluated via several published methods or equations.
These methods are usually based on large population studies, which took skin fold and hydrostatic weighing measurements and then attempt to find equations that manipulate the skin fold measurements so that they match the hydrostatic weighing results.
The reported validity of skin fold measurements is +/-6% at the very best and may be off much more due to several problems with measurement accuracy:
- Inter-operator error, measurements vary widely from technician to technician.
- Technique errors, such as failure to identify the proper measurement site and failure to pinch only fat and no other tissue.
- The underlying assumption that subcutaneous fat represents the same percentage of total fat in every person.
- There are also problems opening skin fold calipers wide enough for very obese persons, resulting in underestimation.
Click on FAQ for more Body Fat related links